
JANE’S LIST
A Platform for Abortion Clinics


OVERVIEW: Jane’s List is a platform designed for abortion clinics to find vetted, pro-choice local vendors. Clinic managers say it has the potential to save them tremendous time and effort, enable them to negotiate better prices, and ultimately can allow clinics to evolve and best serve patients, especially as policy puts the location of clinics in continued flux.
CONTEXT: This project began in a design research course in graduate school. I have continued it onward as a side project, in collaboration with the reproductive justice community.
Research, outreach / recruitment, exploratory interviews, ideation, storyboarding, participatory research, prototyping, UX using behavioral psychology, partnership building
SKILLS:
TEAM:
Initial:
Erica Fink, Elaine Gao, Yifan Zhang
Ongoing:
Erica Fink
Explore the process below or skip through to the final design

I think it’s brilliant. I love the impact for providers. It would be extremely useful.
“
”
– Program Director of a national abortion nonprofit
PROCESS
Stage 1:
Stage 2:
Stage 3:
Stage 4:
Stage 5:
GENERATIVE RESEARCH
Stage 1:
We surveyed 270 abortion healthcare providers (AHPs) and ran in-depth interviews with eight to learn more about key pain points and existing resources.
-
Outreach: To find research participants, we cold emailed clinics across the nation to limited success. Safety and security is a concern in the abortion care field, and proper vetting of outsiders like ourselves is understandably important. After connecting and building trust with a subject matter expert in the field, they offered to share our screener/survey with their network, and our participant pool grew. Relationship building along the way extended our reach.
Criteria: As we screened participants, we heard that clinic administrators may face more of the brunt of stigma and be even less studied than other clinical providers, given they have less prestige. So, we made sure to speak with people involved in an administrative capacity as well as those with clinical experience. We also prioritized speaking with a diverse group of people in red, blue, and swing states. And, we were interested in speaking both with people currently working in abortion care but also with those no longer working in the space, to understand why. -
Of the 270 abortion healthcare providers that we surveyed:
81% have experienced perceived stigma (fear of: rejection, loss of friendship or relationships, criticism, isolation)
68% have experienced experienced stigma (experience of: discrimination, harassment, aggression)
33% have experienced internalized stigma (materialization of: guilt, shame, anxiety)
6% have not experienced abortion-related stigma
We developed our survey question from a description of stigma in the 2018 Reproductive Health journal article: “‘It’s something that marks you’: Abortion stigma after decriminalization in Uruguay” (link)
KEY INSIGHTS:
AHPs face discrimination within the broader medical community.

The geography of abortion care impacts the evolution of services (travel physicians, telehealth etc.)

Extra time and energy is spent trying to find basic local service vendors, from architects to ultrasound techs, who are willing to service clinics.

AHPs face tremendous stress and fear at the prospect of their clinic closing due to election outcomes or changes in policy.

The AHP network is strong but can be difficult to initially access, given vetting requirements and non-mainstream channels.

Humanizing and building connections with providers can normalize abortion.

Abortion procedure is easy to teach, but the soft skills of patient care require nuanced training, the right people, and a strong team dynamic.

AHPs often are torn between their passion for boldly normalizing abortion care and security / safety concerns.

CORE TAKEAWAY: Abortion care providers juggle so much beyond the act of performing abortions — from maintaining clinics, to training volunteers, to navigating the medical field — and each of these responsibilities is made more difficult due to abortion stigma. Even something like finding a plumber for their facilities can be an inordinately challenging task.




CONCEPT DEVELOPMENT
Stage 2:
From our key insights, we identified 24 opportunity areas that we down-selected to five based on potential for impact. We ran “crazy eights” design sprints for solution ideation before narrowing them down and moving forward with three concepts.
-
Opportunity Area: How might we help normalize abortion care as a regular part of a local community by humanizing providers and fostering connection among other healthcare teams and the public?
Why This:Abortion is often made “separate” from other healthcare given stigma and freestanding clinics.
De-stigmatizing abortion within healthcare requires role modeling conversations.
Misinformation spreads more easily without firsthand knowledge.
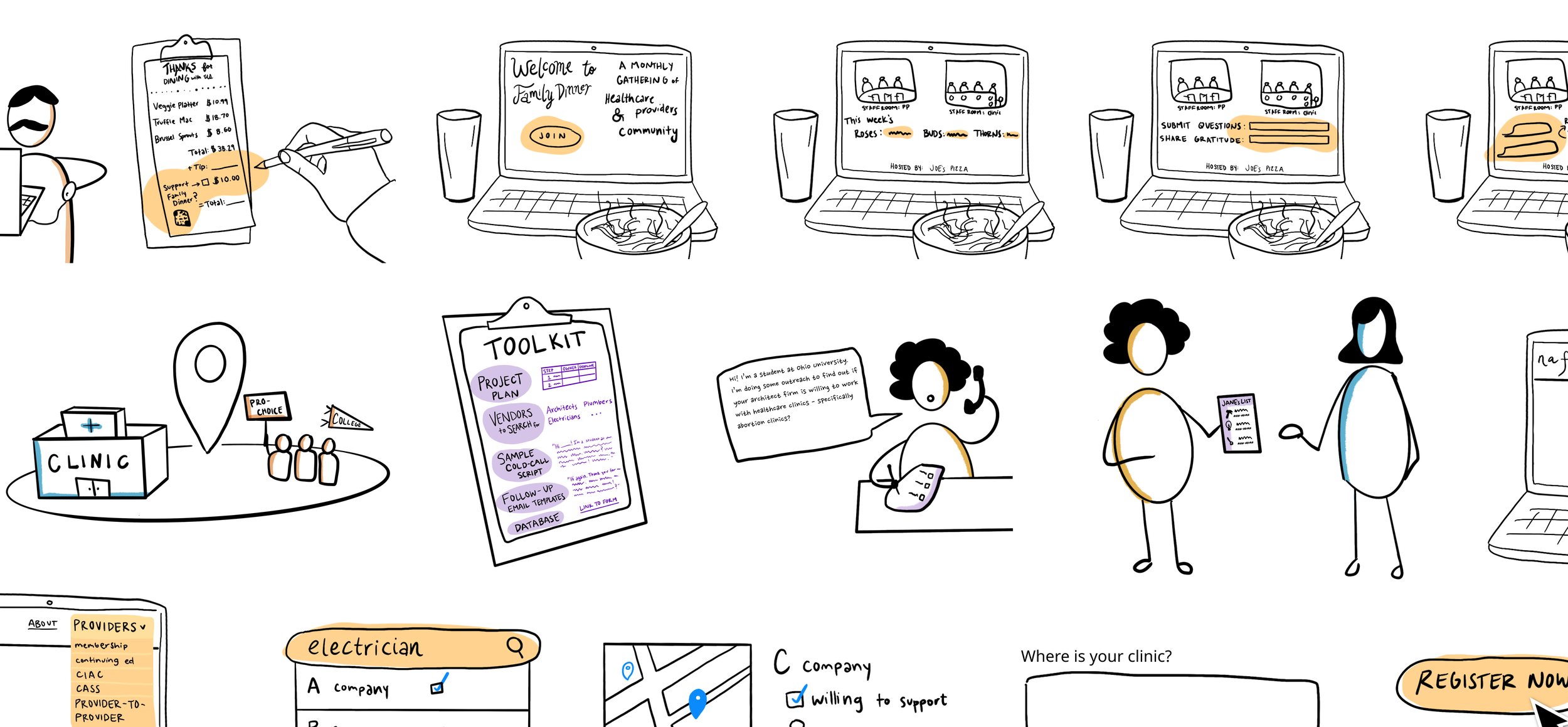
Synopsis: This initiative involves organizing casual events that normalize abortion healthcare providers as regular healthcare providers in their local communities. Proposed sponsors (the American Medical Association and the National Abortion Federation) would together run the initiative, pairing healthcare teams across specialities per-dinner. A local restaurant signs on as a host, excited to attract new customers and show support for local frontline workers. They solicit ticket sales from regular customers in the community in advance by including a purchasable two-part ticket in their menus. The cost of the ticket covers both their attendance and it covers the meal cost of a healthcare provider. The Family Dinner event takes place, and three stakeholder groups break bread together: abortion healthcare providers, other healthcare providers, and community members. Each table has a fishbowl of carefully crafted questions to facilitate conversation for the evening.
-
Opportunity Area: How might we lessen the burden on abortion clinics to find local professional service vendors (architects, accountants, plumbers etc.) who are vetted, pro-choice, and willing to contract for the clinic?
Why This:
Cold calls can take months of time and energy to successfully pan out.
A limited rolodex can lead to price gouging.
The landscape of clinics in America continues to be in flux.
Synopsis: This would be a platform for abortion clinics to find, vet, and share pro-choice contractors and service vendors. It would only be accessible by abortion care providers and live among other provider tools. Clinics can use it two ways: A. searching for a specific need (like an electrician) to see who is already vetted as pro-choice and willing to serve a clinic or B. searching for a specific vendor that they’ve found locally to see if any other clinics have tried working with them and left any reviews. In order to continue accessing information, clinics must leave reviews in return. Local vendors can pro-actively advertise their services in the tool, too.
-
Opportunity Area: How might we lessen the burden on abortion clinics to find local professional service vendors (architects, accountants, plumbers etc.) who are vetted, pro-choice, and willing to contract for the clinic?
Why This:
Cold calls can take months of time and energy to successfully pan out.
A limited rolodex can lead to price gouging.
The landscape of clinics in America continues to be in flux.
SYNOPSIS: This initiative involves enlisting the help of pro-choice university student groups to develop and help maintain a database of supportive local service vendors. An umbrella organization, like the National Abortion Federation (NAF), would ask member clinics if they would want to be partnered with a local, pro-choice college student group. In conjunction with existing student group networks (like Medical Students for Choice and Planned Parenthood Generation Action) the pairings would be made based on proximity. Students would attend virtual training sessions, gain a vetting toolkit with a project plan, types of vendors to search for, a sample cold-call script, follow-up email templates, and a form to build the database. After students build the list, the clinic can choose to request ongoing help maintaining it and the door is opened for greater involvement and volunteering.
We developed these ideas into medium-fidelity storyboards to use in our next round of research.

EVALUATIVE RESEARCH
Stage 3:
We next met with four providers in different contexts to learn what elements of our three concepts worked, what didn’t, and to iterate on our solutions.
-
Sample Structure:
Build rapport through introductions
Share context to our research and pause to validate our learnings thus far
Workshop each concept:
see how the opportunity area resonates
walk through the storyboard
solicit overall feedback and gut reactions
gather detailed feedback for each step in an idea’s process
run exercises like “build it, break it, fix it”
From these interviews, we:
validated: (A) the challenge of finding local vendors (B) interest in volunteer and student involvement made easier through onboarding support.
learned: (A) specific details for what should go into the vetting process (B) who the right partners are (C) when volunteer efforts are impactful (D) what elements of a review would most benefit providers and be easy to fill out (E) what safety concerns exist digitally for clinics.
pivoted: away from the “Family Dinner Event Series,” given substantial safety concerns that require extensive iteration on the idea.
newly considered: combining the “Student Rolodex Initiative” and “Provider-to-Provider Platform.”
and prioritized: staying inclusive of scenarios where clinics are most isolated or stigmatized.

FINAL OUTCOME
Jane’s List is a digital platform designed to save clinics time, money, and effort by enabling administrators to better vet local service vendors (handymen, electricians, cleaning services, etc.) and share knowledge with one another.
Following our user interviews, we chose to focus on this challenge of vetting vendors — the opportunity with the most tangible traction toward impact.
We designed the platform to:
serve abortion clinics in various contexts (rural or urban; highly stigmatized or not; newly opened or long-standing, etc.)
be secure and accessible for clinics given safety concerns, following in the footprints of tools in this space like CASS
enable local coalition building with other progressive organizations facing similar challenges due to stigma
to lessen the burden on administrators through a data-driven vetting guide that can empower pro-choice student groups and volunteers to support local clinics
WHY THE NAME “JANE’S LIST”?
“Jane” references the underground collective of activists in Chicago that, despite the risk of felony, provided access to abortions between 1969 to 1973, prior to Roe vs. Wade.
Providers to this day continue to act in bravery to provide people safe, affordable abortion access in a country that constantly threatens this basic human right of healthcare.
If Jane’s List were to exist — we would hope that by logging in, providers could feel a sense of support from a tool designed for them. They are seen and appreciated by many.
FEATURE 1: REVIEW SHARING
The primary feature of Jane’s List is the ability to read and share reviews of local vendors among abortion clinics. This can cut down on the time and effort that administrators spend on vetting and increase their ability to negotiate prices.
Review sharing serves clinics in areas where there are multiple clinics — sometimes even 15 minutes apart — that are already knowledge sharing:
"There's another abortion clinic in [our state] that we talk to pretty frequently. And so we ended up just sharing information back and forth. But it would be very helpful to have more than just them and to have more than just like texting each other being like, ‘Hey, did this company work for you?’"
- interview quote from clinic administrator in the Northeast
It also serves clinics that are newly opening and don’t have these local relationships yet. Given the volatility of abortion policy in America, the landscape of clinics continues to be in flux. Providers are moving to new states to open clinics after being forced to close in their hometowns. They can benefit from local knowledge — either from nearby clinics or a clinic that closed years prior.
But, we also know that some regions may only have one clinic. Our solution needs to account for ways to serve these clinics too. So, we designed the next feature for coalition building.

FEATURE 2: COALITION BUILDING
A member clinic can choose to invite partners — specifically other progressive, stigmatized organizations in their region — to access and use Jane’s List.
Addressing this solution with intersectionality can lead to better outcomes for all.
“Getting ally organizations being able to use that tool as well, I could absolutely see more of a benefit. Especially in the more red isolated, maybe even rural areas. Those organizations tend to have less support.”
- interview quote from former Director of Patient Advocacy at a clinic in the Deep South
FEATURE 3: VETTING GUIDE
Another type of partner for Jane’s List is advocacy groups and pro-choice college student groups, who can help maintain and build the database of vetted vendors.
Logged in as this specific type of user, volunteers have limited access to Jane’s List and specifically can only vet a vendor and access the platform’s vetting guide.
The Vetting Guide is a step-by-step resource that would be developed by a provider committee to include:
onboarding videos
sample call scripts and follow-up email templates
additional best practices for vetting local vendors
emotional reassurance through member stories to support anyone doing outreach if they inevitably speak to someone who is anti-abortion
a data-driven dashboard that pinpoints top vetting needs according to region and vendor type
Each of these features is intentional to maximize the use of a volunteer’s time and to minimize the time clinic staff need to onboard volunteers.
REDUCING FRICTION USING BEHAVIORAL SCIENCE
Jane’s List can model some of its UX/UI off of existing review platforms (to not reinvent the wheel and use up precious funding).
Still, the success of Jane’s List would rely heavily on its usability for this specific use case. Clinic administrators are beyond capacity — so Jane’s List must be designed with limited attention in mind and with as little friction for the user as possible.
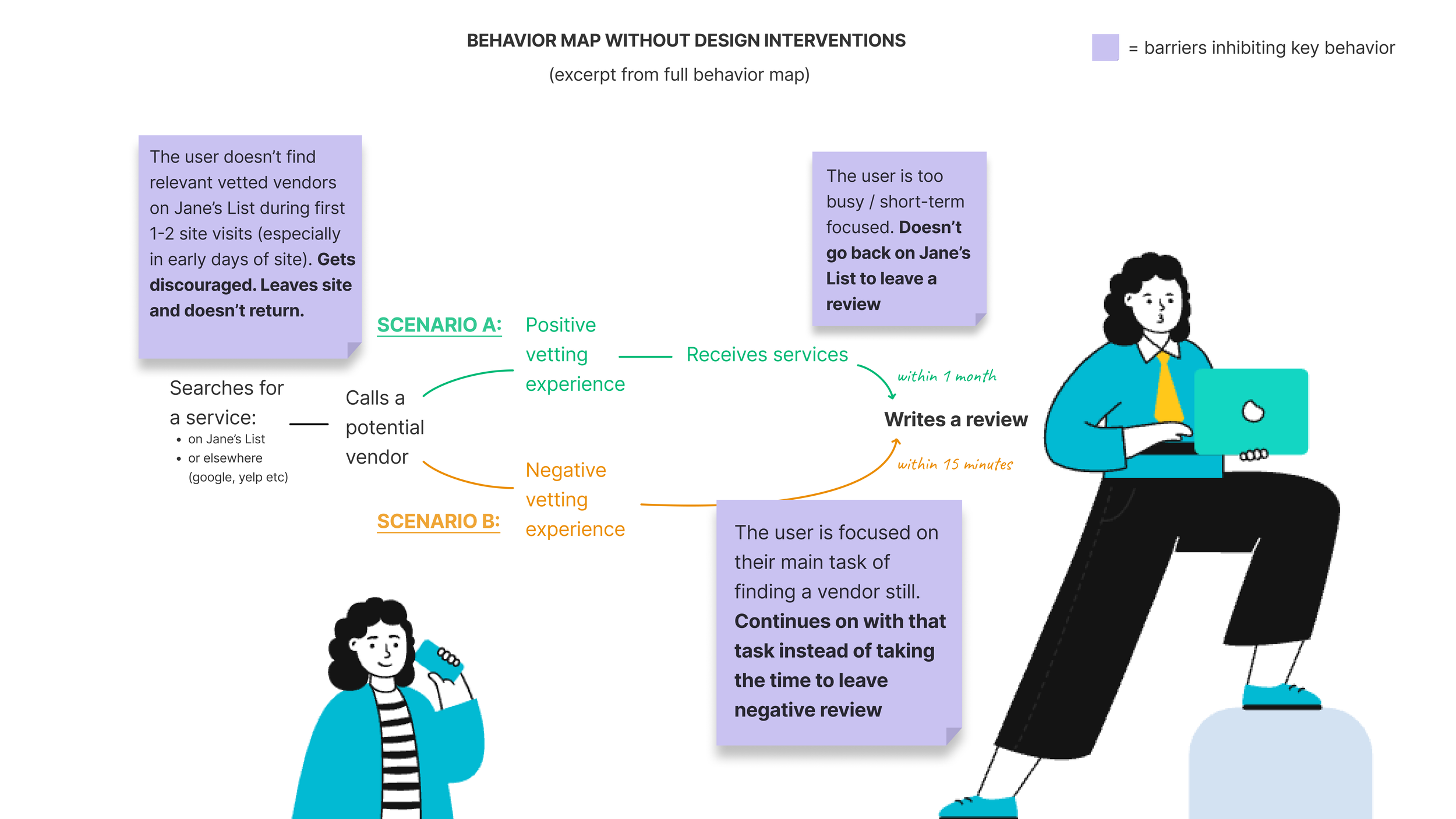
I created a behavior map to identify a user’s potential barriers and designed interventions to improve adoption of the tool.
For instance: what if a user’s search yields “no results”?
Especially when the database is growing in the early days, this may happen often. Jane’s List risks losing that user due to negativity bias. To mitigate this risk, I’ve made it so the user knows that they’re being heard through transparency that their search query has been flagged for volunteers to proactively find. I’ve also added a default for them to receive an email when results for their search are added to the database.
FURTHER EXPLORATION
Based on the potential for impact and positive feedback from providers thus far, I would love to further develop this project.
Next steps would include:
Interviewing vendors. Even pro-choice vendors can face difficulty servicing abortion clinics due to TRAP laws which place “unnecessary regulations, personnel qualifications building and/or structural requirements” on clinics. Architects and other types of vendors may benefit from a “Resource Hub” of sorts through Jane’s List to more easily service clinics and ultimately join advocacy to dismantle TRAP laws.
Validating feature #2. I would like to talk with coalitions and other progressive, stigmatized organizations to better understand how Jane’s List would serve them.
Connecting with potential sponsors. Providers repeatedly described the Abortion Care Network as a strong potential sponsor of Jane’s List. Their feedback and potential partnership would be invaluable.